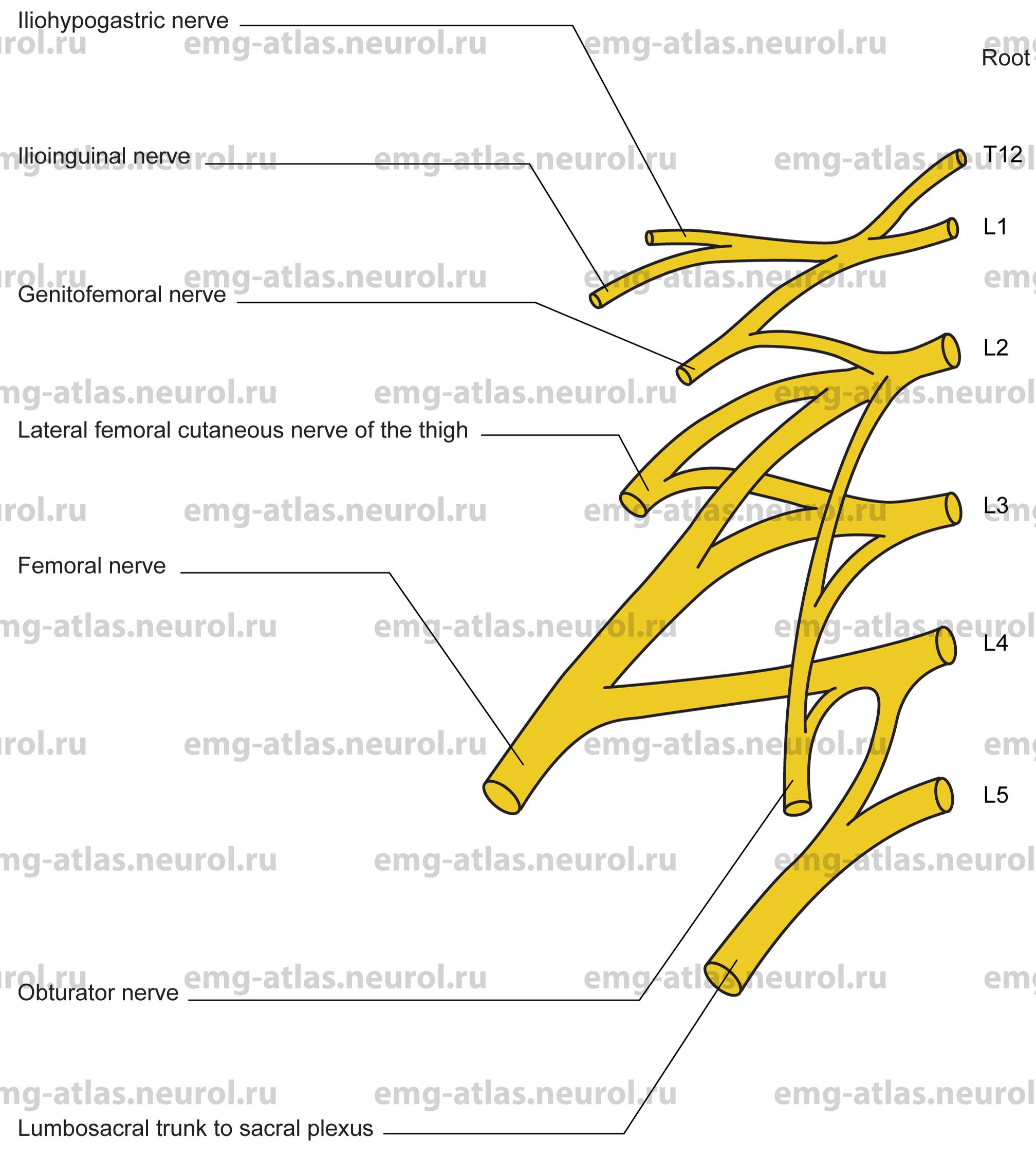
Diagram of the lumbar plexus (anterior view) and its branches.
The lumbar plexus is formed by the first three and most of the fourth lumbar ventral rami; the smaller branch of the fourth joins the fifth as the lumbosacral trunk, which joins the sacral plexus (see chapter 14). Although the fourth lumbar ventral ramus is most often divided between the two plexuses, in a prefixed plexus the third may be the divided ramus whereas in a postfixed plexus the fifth ramus contributes to both plexuses. These variations modify the lumbar and sacral plexuses (Gray’s Anatomy, 1995).
The lumbar ventral rami descend laterally into the psoas major muscle to form the lumbar plexus. In its usual arrangement, the first lumbar ventral ramus, often joined by a branch from the twelfth thoracic, bifurcates into upper and lower parts. The upper part divides again into iliohypogastric and ilio-inguinal nerves; the lower unites with a branch of the second lumbar ramus to form the genitofemoral nerve. The remainder of the second and third and part of the fourth lumbar ventral rami joining the plexus divide into ventral (anterior) and dorsal (posterior) divisions. The anterior division of the second to fourth ventral rami form the obturator nerve. The posterior division of the second to fourth ventral rami form the femoral nerve. Posterior branches of the second and third ventra rami also form the lateral femoral cutaneous nerve of the thigh. Muscular branches of the lumbar plexus directly supply the quadratus lumborum, psoas minor, psoas major, and iliacus (the latter also receives innervation from the femoral nerve). The iliohypogastric nerve contributes innervation to the transversus abdominis and to the internal and external oblique muscles. It then supplies cutaneous sensation to the posterolateral gluteal skin and the suprapubic skin. The ilio-inguinal nerve also contributes innervation to the transversus abdominis and internal oblique muscles. It traverses the inguinal canal and emerges from the superficial inguinal ring to supply the proximomedial skin of the thigh and the skin covering the penile root and upper scrotm or that covering the moms pubis and the adjoining labium majus. The genital branch of the genitofemoral nerve supplies the cremaster muscle and provides cutaneous innervation to the scrotal skin in men or to the moms pubis and labium majus in women. The femoral branch supplies the skin over the upper part of the femoral triangle. Injury to the iliohypogastric, ilio-inguinal, and genitofemoral nerves is almost always the result of direct trauma, usually related to surgery (inguinal herniorrhaphy or retrocaecal appendix).
The lateral femoral cutaneous nerve of the thigh descends behind the inguinal ligament about 1 cm medial to the anterior superior iliac spine. It divides into anterior and posterior branches, the former supplying skin over the anterior and lateral thigh as far as the knee and the latter supplying skin on the lateral surface of the thigh from the greater trochanter to about midthigh. A lesion of the lateral femoral cutaneous nerve, usually due to compression behind the inguinal ligament, produces impaired sensation with pain and paraesthesias on the anterior and lateral aspects of the thigh. This condition is known clinically as meralgia paraesthetica.
A lesion of the lumbar plexus produces a clinical picture similar to that seen with combined femoral and obturator nerve lesions, but with additional involvement of the above-mentioned branches. It is common for femoral nerve deficit to be accompanied by obturator nerve deficit (Dawson et al., 1990) because both arise within the substance of the psoas muscle. The femoral and obturator nerves are discussed individually.