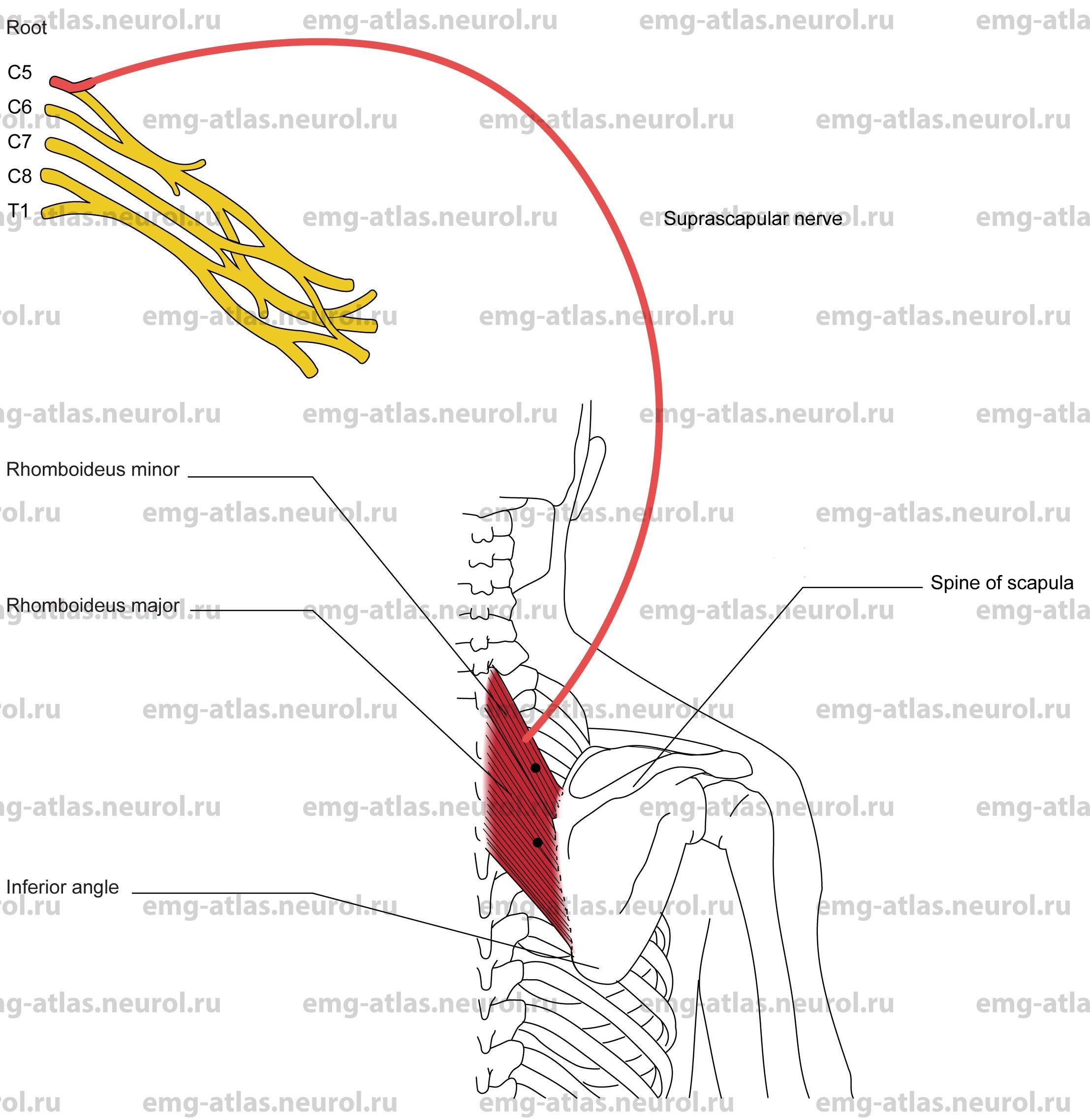
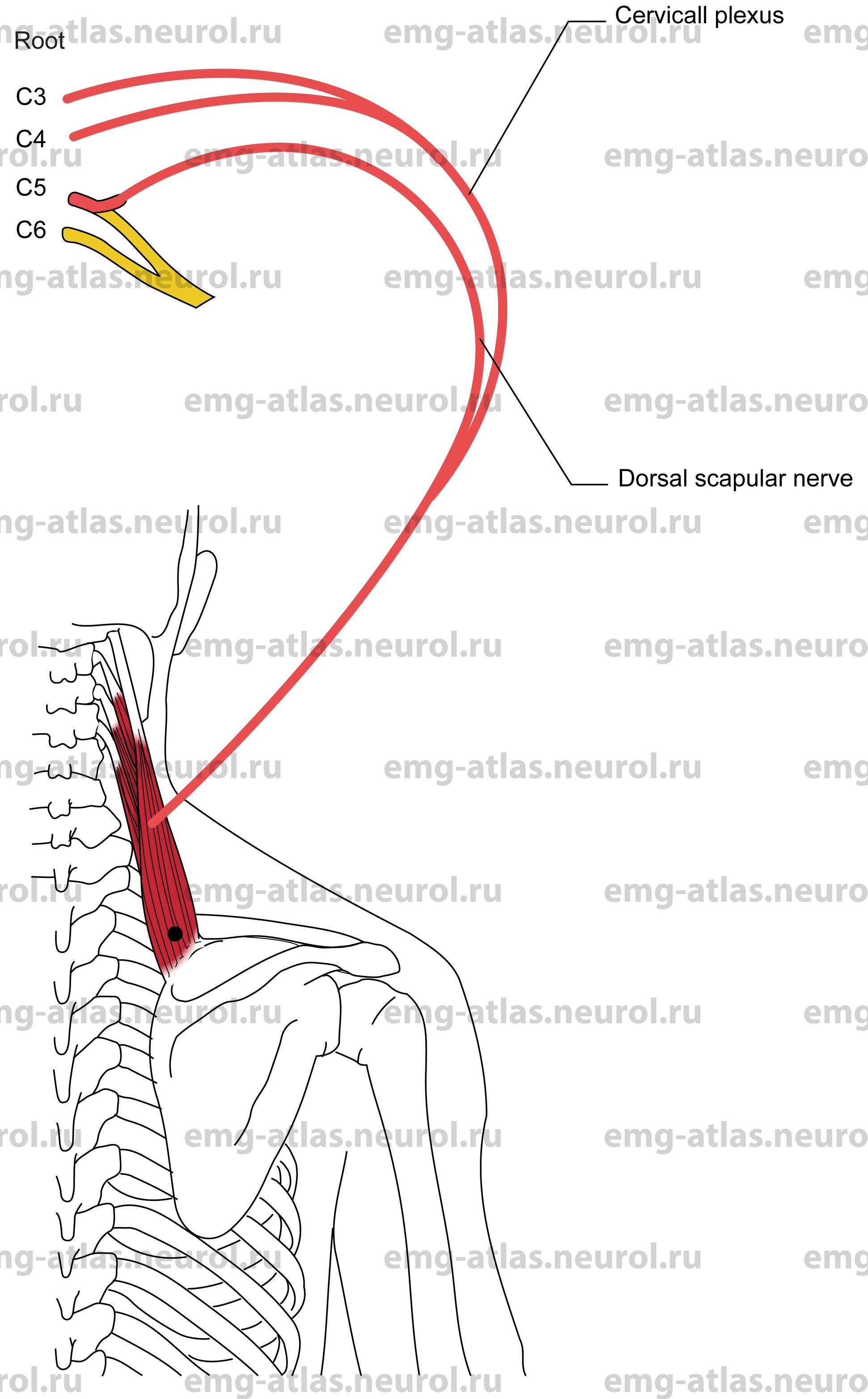
The dorsal scapular nerve originates predominantly from the fifth cervical spinal nerve within the substance of the scalenus medius muscle, but it may receive additional fibers from the fourth and sixth spinal nerves. (Gray’s Anatomy, 1995). It may arise in conjunction with the upper root of the long thoracic nerve (Sunderland, 1968). The nerve courses behind the brachial plexus and descends obliquely through the scalenus medius to reach the deep surface of the levator scapulae muscle. It usually sends a twig to this muscle, which receives most of its nerve supply from the third and fourth cervical roots. The nerve continues downward along the medial margin of the scapula to innervate the rhomboideus major and rhomboideus minor muscles (rhomboids).
Dorsal Scapular Nerve Lesion
Etiology
Trauma to the back and penetrating wounds can cause direct nerve injury.
Rarely, entrapment due to hypertrophy of the scalenus medius muscle (Kopell and Thompson, 1976) causes a dorsal scapular nerve lesion.
General Comments
Isolated lesions of this nerve are rare.
Clinical Features
Possible shoulder pain is most marked along the medial border of the scapula.
Wasting of the rhomboid muscles produces slight winging of the scapula.
There is difficulty drawing the scapula directly backward toward the spine. It is questionable whether an isolated nerve lesion would be clinically recognized (Sunderland, 1968) because the trapezius muscle will compensate for paralysis of the rhomboids and levator scapulae.
Electrodiagnostic Strategy
Demonstrate neurogenic EMG changes in the rhomboids and levator scapulae.
Exclude C5 radiculopathy by performing EMG in other C5 muscles. Note: Because isolated lesions of this nerve are rare, neurogenic EMG changes in rhomboids or levator scapulae usually imply C5 radiculopathy.
Perform nerve conduction studies to exclude an upper trunk lesion.
Anatomical Illustrations
Rhomboideus Major and Minor
Innervation
Innervation is via the dorsal scapular nerve and root C5.
Origin
The major rhomboideus originates at the spinous processes of the second to fifth thoracic vertebrae.
The minor rhomboideus originates at the spinous processes of the seventh cervical and first thoracic vertebrae.
Insertion
Major: Insertion is at the medial scapular border between the inferior angle and the spine of the scapula.
Minor: Insertion is at the medial scapular border at the base of the spine of the scapula.
Activation Maneuver
Retraction of the scapula (drawing the scapula directly backward toward the vertebral spine) activates the muscles. EMG Needle Insertion
Major: Insert the needle just medial to the medial margin of the scapula, midway between the scapular spine and the inferior angle.
Minor: Insert the needle just medial to medial border of the scapular spine.
Pitfalls
Major and minor: If the needle is inserted too superficially, it will be in the trapezius muscle, which is supplied by the spinal accessory nerve.
Major only: If the needle is inserted too caudad and superficially, it may be in the latissimus dorsi, which is supplied by the thoracodorsal nerve.
Pneumothorax following needle examination has been reported in the literature (Miller, 1990).
Clinical Comments
Neurogenic changes in the rhomboids on needle examination usually indicate a C5 radiculopathy.
Look for neurogenic changes in other C5-innervated muscles.
Anatomical Illustrations
Levator Scapulae
Innervation
Innervation is via the anterior rami of C3, C4, and Cs, the latter branch via the dorsal scapular nerve.
Origin
The levator scapulae originate at the transverse processes of the upper four cervical vertebrae.
Insertion
Insertion is at the posteromedial border of the scapula, between the superior angle and the spine of the scapula.
Activation Maneuver
Elevation of the scapula (which assists the trapezius in shrugging shoulders) activates the levator scapulae. EMG Needle Insertion
Insert the needle along the superomedial margin of the scapula.
Pitfalls
If the needle is inserted too superficially, it will be in the trapezius muscle, which is supplied by C3 and C4 spinal nerves and the spinal accessory nerve.
If the needle is inserted too deeply, it may be in the paraspinal muscles, which are supplied by the posterior rami of the spinal nerves.
Clinical Comments
Neurogenic changes in this muscle on needle examination usually indicate a C3-C5 radiculopathy.
Look for neurogenic changes in other C3-C5 innervated muscles to confirm radiculopathy.