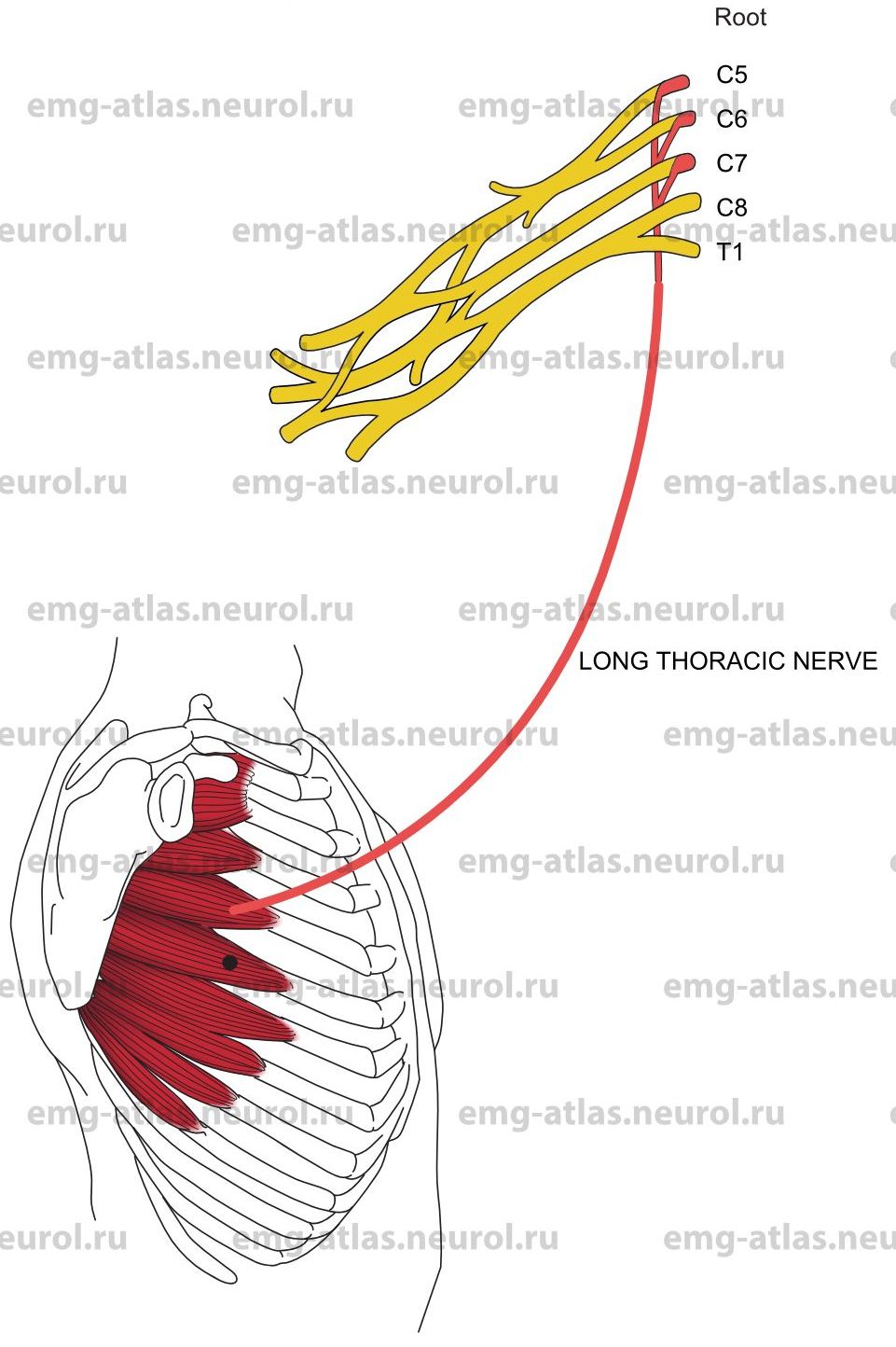
The long thoracic nerve is formed by roots from the fifth to the seventh cervical rami (Gray’s Anatomy, 1995). The upper two roots pierce the scalenus medius obliquely, unite within the muscle, and are then joined by the seventh root, which runs anterior to this muscle. The nerve descends posterior to the brachial plexus, crosses the outer border of the first rib, and descends further along the outer thoracic wall on the surface of the serratus anterior muscle. It supplies this muscle by filaments passing to the several digitations of the muscle.
Long Thoracic Nerve Lesion
Etiology
Trauma to the posterior triangle of the neck causes direct nerve injury. Traction injury occurs when the angle between the neck and the shoulder is forcibly increased (Sunderland, 1968).
Rarely, entrapment due to hypertrophy of the scalenus medius muscle causes a long thoracic nerve lesion (Kopell and Thompson, 1976).
Neuralgic amyotrophy is causative. Winging of the scapula may be the only manifestation of neuralgic amyotrophy (Gray’s Anatomy, 1995).
General Comments
Because the nerve is attached to the scalenus medius above and the serratus anterior below, the nerve is susceptible to stretch injury when the shoulder or chest wall is depressed or the neck is flexed to the opposite side.
Clinical Features
Pain that is dull aching in quality is most marked along the shoulder. Weakness of the serratus anterior produces prominent winging scapula. This is easily demonstrated by asking the patient to push against resistance with the arm extended at the elbow and forward flexed to 90 degrees at the shoulder.
Electrodiagnostic Strategy
Demonstrate neurogenic EMG changes in the serratus anterior. Exclude C5, C6 or C7 radiculopathy by performing EMG in other muscles. Perform nerve conduction studies to exclude a brachial plexus lesion.
Anatomical Illustrations
Serratus Anterior
Innervation
Innervation is via the long thoracic nerve and roots C5, C67, C7.
Origin
The serratus anterior originates at the outer surfaces and superior borders of the upper eight or nine ribs.
Insertion
Insertion is at the medial border of the scapula, from the superior angle to the costal surface of the inferior angle.
Activation Maneuver
Forward flexion of the arm and pushing against resistance activate the muscle.
EMG Needle Insertion
Insert the needle along midaxillary line directly over the rib, anterior to the bulk of the latissimus dorsi but, in a woman, posterior to breast tissue. Palpating the interspace on either side can isolate a single rib. The serratus anterior is the only muscle between the skin and the rib.
Pitfalls
Pneumothorax following needle examination of the serratus anterior has been reported (Johnson and Parker, 1980).
Clinical Comments
Neurogenic EMG changes limited to the serratus anterior suggest an isolated lesion of the long thoracic nerve.
EMG of other C5, C6 or C7 muscles should be performed to exclude radiculopathy.